Hydrocephalus
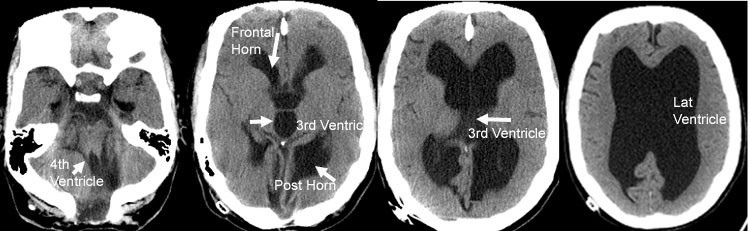
The brain sits inside the skull floating in fluid called CSF (Cerebrospinal Fluid). This fluid is made inside cavities in the brain called ventricles. There are 4 ventricles in the brain; two lateral ventricles, the third ventricle and the fourth ventricle. CSF flows from the lateral ventricles to the third ventricle, then via a channel called the cerebral aqueduct (of Sylvius) to the fourth ventricle. The CSF leaves the ventricles via 3 openings in the fourth ventricle; the midline foramen of Magendie and the two side openings called the foramena of Luschka. From there, the CSF travels in a space over the surface of the brain called the subarachnoid space. The CSF travels over the brain and spinal cord, before being absorbed in the large veins in the skull.
CSF circulation is continuous, with the brain producing approximately 20 ml CSF every hour. Because the volume of the skull is fixed, the production of CSF has to be balanced by absorption of CSF. Any imbalance in the production-absorption system leads to significant problems.
CSF circulation is continuous, with the brain producing approximately 20 ml CSF every hour. Because the volume of the skull is fixed, the production of CSF has to be balanced by absorption of CSF. Any imbalance in the production-absorption system leads to significant problems.
Any build-up of CSF in the ventricles is called hydrocephalus. In general, there are two forms of hydrocephalus: (i) communicating hydrocephalus and (ii) non-communicating hydrocephalus.
Communicating hydrocephalus
In this form of hydrocephalus, the CSF is free to travel throughout the ventricles and subarachnoid space. Thus, the ventricles and subarachnoid space communicate. The problem in communicating hydrocephalus is either over-production of CSF, or more commonly, decreased absorption of CSF. Any condition that obstructs flow of CSF into the veins for absorption causes communicating hydrocephalus. Some common examples of such causes are meningitis, traumatic brain haemorrhage, subarachnoid haemorrhage, brain tumours and infection.
Non-communicating hydrocephalus
If there is an obstruction to flow of CSF in the ventricles, or from the fourth ventricle to the subarachnoid space, then there is a CSF build-up in the ventricular system, causing non-communicating hydrocephalus. There are many causes of non-communicating hydrocephalus including tumours, colloid cysts, arachnoid cysts, membranous webs and aqueduct stenosis.
Symptoms of hydrocephalus are due to raised intracranial pressure, including
In infants, hydrocephalus can produce skull enlargement (increased head circumference), failure to thrive, seizures, downward deviation of the eyes (sunset eyes), and prominence of the scalp veins.
In the elderly population, there is a condition known as normal pressure hydrocephalus (NPH) that classically presents with walking difficulty, bladder incontinence and memory problems.
The diagnosis of hydrocephalus is based on the history and examination findings, in addition to a brain scan. CT scan will confirm the presence of enlarged ventricles, but MRI is most useful because it can identify many of the possible causes of hydrocephalus. In infants, ultrasound may be used.
Treatment of hydrocephalus depends on the cause and type of hydrocephalus. When the cause is something like a tumour blocking the flow of CSF, then removal of the tumour will often cure the hydrocephalus.
In this form of hydrocephalus, the CSF is free to travel throughout the ventricles and subarachnoid space. Thus, the ventricles and subarachnoid space communicate. The problem in communicating hydrocephalus is either over-production of CSF, or more commonly, decreased absorption of CSF. Any condition that obstructs flow of CSF into the veins for absorption causes communicating hydrocephalus. Some common examples of such causes are meningitis, traumatic brain haemorrhage, subarachnoid haemorrhage, brain tumours and infection.
Non-communicating hydrocephalus
If there is an obstruction to flow of CSF in the ventricles, or from the fourth ventricle to the subarachnoid space, then there is a CSF build-up in the ventricular system, causing non-communicating hydrocephalus. There are many causes of non-communicating hydrocephalus including tumours, colloid cysts, arachnoid cysts, membranous webs and aqueduct stenosis.
Symptoms of hydrocephalus are due to raised intracranial pressure, including
- headache
- nausea and vomiting
- confusion
- drowsiness
- double vision
- balance problems
In infants, hydrocephalus can produce skull enlargement (increased head circumference), failure to thrive, seizures, downward deviation of the eyes (sunset eyes), and prominence of the scalp veins.
In the elderly population, there is a condition known as normal pressure hydrocephalus (NPH) that classically presents with walking difficulty, bladder incontinence and memory problems.
The diagnosis of hydrocephalus is based on the history and examination findings, in addition to a brain scan. CT scan will confirm the presence of enlarged ventricles, but MRI is most useful because it can identify many of the possible causes of hydrocephalus. In infants, ultrasound may be used.
Treatment of hydrocephalus depends on the cause and type of hydrocephalus. When the cause is something like a tumour blocking the flow of CSF, then removal of the tumour will often cure the hydrocephalus.
Non-communicating hydrocephalus
The treatment of choice for this type of hydrocephalus is neuro-endoscopic third ventriculostomy (NETV). This involves insertion of a small telescope into the third ventricle, where a small hole is created to allow CSF to flow directly into the subarachnoid space, without the need for the CSF to travel through the aqueduct and fourth ventricle. This procedure provides excellent long term results, without the need for insertion of any synthetic material. Professor Gavin Davis has significant expertise with this technique, and will recommend this procedure for you if the clinical presentation and MRI findings indicate that you are a suitable candidate for NETV.
The treatment of choice for this type of hydrocephalus is neuro-endoscopic third ventriculostomy (NETV). This involves insertion of a small telescope into the third ventricle, where a small hole is created to allow CSF to flow directly into the subarachnoid space, without the need for the CSF to travel through the aqueduct and fourth ventricle. This procedure provides excellent long term results, without the need for insertion of any synthetic material. Professor Gavin Davis has significant expertise with this technique, and will recommend this procedure for you if the clinical presentation and MRI findings indicate that you are a suitable candidate for NETV.
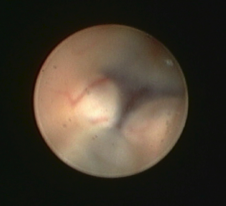
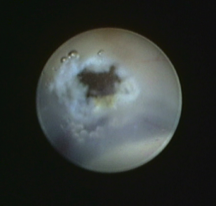
Images demonstrating the neuro-endoscopic view of the floor of the third ventricle (left), and following creation of the fenestration in the floor of the ventricle (right).
Communicating hydrocephalus
The treatment for this type of hydrocephalus is insertion of a shunt, most commonly a ventriculo-peritoneal shunt (VP Shunt). (see images below) This involves insertion of a plastic tube into the ventricle, and connecting the tube to a one-way valve that sits under the skin, often behind the ear. The valve is then connected to another plastic tube (peritoneal catheter) that lies under the skin between the head and the abdomen, where it then enters the abdomen to the cavity known as the peritoneum, sitting between the bowels and other abdominal organs. The CSF then travels down the tube, via the valve into the peritoneal cavity where it is then absorbed. Modern shunts can be very effective, and come in many shapes and styles. However, as they are synthetic prostheses, they are at risk of infection, malfunction and blockage. When this occurs, the shunt needs to be replaced with another operation. Some people with shunts require frequent surgery to replace shunts, whilst some shunts may last years before needing replacement.
NPH
The treatment of choice for NPH is insertion of a VP shunt, although occasionally NETV has demonstrated benefit in some patients.
The treatment for this type of hydrocephalus is insertion of a shunt, most commonly a ventriculo-peritoneal shunt (VP Shunt). (see images below) This involves insertion of a plastic tube into the ventricle, and connecting the tube to a one-way valve that sits under the skin, often behind the ear. The valve is then connected to another plastic tube (peritoneal catheter) that lies under the skin between the head and the abdomen, where it then enters the abdomen to the cavity known as the peritoneum, sitting between the bowels and other abdominal organs. The CSF then travels down the tube, via the valve into the peritoneal cavity where it is then absorbed. Modern shunts can be very effective, and come in many shapes and styles. However, as they are synthetic prostheses, they are at risk of infection, malfunction and blockage. When this occurs, the shunt needs to be replaced with another operation. Some people with shunts require frequent surgery to replace shunts, whilst some shunts may last years before needing replacement.
NPH
The treatment of choice for NPH is insertion of a VP shunt, although occasionally NETV has demonstrated benefit in some patients.


Left:
Schematic view of a shunt system in place.
Above:
Close up view of a programmable shunt valve.