Thoracic Outlet Syndrome
Thoracic outlet syndrome (TOS) causes nerve compression resulting in pain, numbness and weakness in the hand.
There are 3 types of TOS classically described, although only the first two are truly TOS:
This page is specific to type I, or Neurogenic TOS.
Vascular TOS is a different condition that causes compression of the subclavian artery or vein, and is best treated by vascular surgeons.
Type III, or disputed TOS, is not really TOS, but is often mistakenly called TOS by doctors and therapists because of the presence of a cervical rib. It should be noted that up to 3% of the normal population have a cervical rib, and do not have TOS. Cervical rib does not cause neurogenic TOS.
There are 3 types of TOS classically described, although only the first two are truly TOS:
- Neurogenic TOS
- Vascular TOS
- Disputed or Non-specific TOS
This page is specific to type I, or Neurogenic TOS.
Vascular TOS is a different condition that causes compression of the subclavian artery or vein, and is best treated by vascular surgeons.
Type III, or disputed TOS, is not really TOS, but is often mistakenly called TOS by doctors and therapists because of the presence of a cervical rib. It should be noted that up to 3% of the normal population have a cervical rib, and do not have TOS. Cervical rib does not cause neurogenic TOS.
The Thoracic Outlet
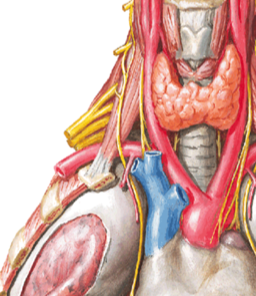
This term confuses many people. In its simplest form, it refers to the area between the neck, the chest and the shoulder.
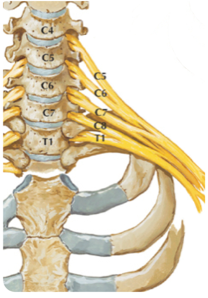
This area is important because many critical nerves and blood vessels travel through it. The structures of importance to the Neurosurgeon in TOS are the major nerves from the neck that supply the hand.
These nerves travel in the brachial plexus; the nerves that are most affected in TOS are the C8 and T1 nerves, in addition to the lower trunk of the brachial plexus.
This term confuses many people. In its simplest form, it refers to the area between the neck, the chest and the shoulder.
This area is important because many critical nerves and blood vessels travel through it. The structures of importance to the Neurosurgeon in TOS are the major nerves from the neck that supply the hand.
These nerves travel in the brachial plexus; the nerves that are most affected in TOS are the C8 and T1 nerves, in addition to the lower trunk of the brachial plexus.
Neurogenic Thoracic Outlet Syndrome
TOS results from compression of the C8/T1/Lower trunk by a fibrous band.
This results in dysfunction of the nerves, and produces:
TOS results from compression of the C8/T1/Lower trunk by a fibrous band.
This results in dysfunction of the nerves, and produces:
- pain in the hand
- numbness in the hand and fingers
- weakness of the hand muscles
- wasting of the hand muscles (see picture on right)

Diagnosis and Investigations
The diagnosis of neurogenic TOS requires clinical assessment by an expert in TOS, including the appropriate clinical history and examination findings.
If TOS is suspected, then Investigations performed include:
Nerve Conduction Studies and EMG - an electrical test to measure nerve function
MRI of the cervical spine and brachial plexus, to exclude other potential causes. It should be noted that in most cases of TOS, the MRI will be normal. The presence of a cervical rib is irrelevant, because TOS is due to fibrous bands compressing the nerves.
The diagnosis of neurogenic TOS requires clinical assessment by an expert in TOS, including the appropriate clinical history and examination findings.
If TOS is suspected, then Investigations performed include:
Nerve Conduction Studies and EMG - an electrical test to measure nerve function
MRI of the cervical spine and brachial plexus, to exclude other potential causes. It should be noted that in most cases of TOS, the MRI will be normal. The presence of a cervical rib is irrelevant, because TOS is due to fibrous bands compressing the nerves.
Treatment
The treatment of TOS depends on the symptoms, signs and severity. Very mild cases are initially treated with conservative measures.
In the presence of muscle weakness/wasting, or pain with confirmatory NCS/EMG, surgery is required.
Surgery involves an incision above the collarbone; dissection of the brachial plexus nerves; division of any membranes compressing the nerves.
As with all operations, there are risks involved, including injury to nerves, major blood vessels and the lung, in addition to anaesthetic risks.
Overall, the success rate from surgery is usually good.
To discuss the surgery results and risks in more detail, please make an appointment with Prof Davis.
The treatment of TOS depends on the symptoms, signs and severity. Very mild cases are initially treated with conservative measures.
In the presence of muscle weakness/wasting, or pain with confirmatory NCS/EMG, surgery is required.
Surgery involves an incision above the collarbone; dissection of the brachial plexus nerves; division of any membranes compressing the nerves.
As with all operations, there are risks involved, including injury to nerves, major blood vessels and the lung, in addition to anaesthetic risks.
Overall, the success rate from surgery is usually good.
To discuss the surgery results and risks in more detail, please make an appointment with Prof Davis.